|
|
|
Jarrod Shapiro, DPM
Practice Perfect Editor
Assistant Professor,
Dept. of Podiatric Medicine,
Surgery & Biomechanics
College of Podiatric Medicine
Western University of
Health Sciences,
St. Pomona, CA |
Part 1
Lately, I’ve had a run of patients on the larger side of the weight spectrum. I’m sure it’s really not a “lately” issue but rather my happening to focus attention on this aspect. It seems that almost every plantar fasciitis patient of mine is obese. This isn’t unique, I know, but when my medical assistants tell me about a new patient they’ve just roomed complaining of “heel pain, the first thing I think of is plantar fasciitis. I try to remain cognizant of the entire differential diagnosis of heel pain, but it seems invariably once I walk into the room, hear the classic history, and do my physical exam, my first predictions of plantar fasciitis are correct. The problem I have, though, is not with the diagnosis but rather with the fact that the one major contributing factors to these patients – their obesity – is the one factor on which we in the medical profession have the least effect.
Epidemiology
Just as a quick reminder, the spectrum of obesity is defined using BMI
(body mass index or mass in kg/height in m2).1
For adults, the scale is as follows:
Underweight: < 18.5
Healthy weight:18.5 – 24.9
Overweight: 25-29.9
Obese: ≥ 30
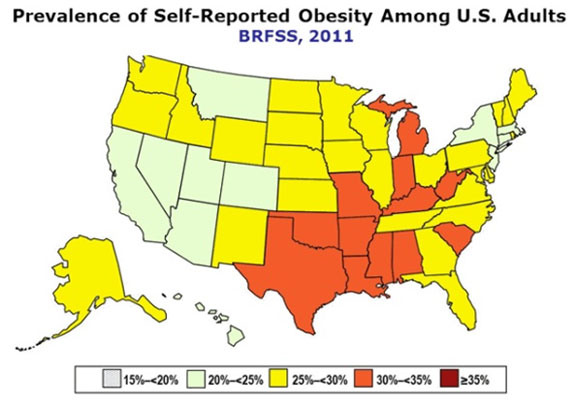
How big is this problem that potentially affects all of us? According to the Centers for Disease Control and Prevention more than 35% of adults and 17% of children were obese in 2009-2010 (2). This translates to over 78 million adults in the United States.2 Since a picture’s worth a thousand words, take a look at the figure below which shows the prevalence of self-reported obesity in the US.3 The South has the highest prevalence. Who could blame them with all that delicious fried food? Mississippi has the highest prevalence at 34.9%, with Louisiana running a close second (33.4%).3 Interestingly, even the areas with the lowest prevalence are no lower than 20%. We’re an overweight country.
For disclosure’s sake, I’m 5 feet, 7 inches and 170 pounds which makes my BMI 26.6, putting me in the overweight category. Although I’m a bit low on the scale, I am technically one of the very people I’m commenting about. To add a sense of the personal nature of this problem, I have a history of symptomatic pes planus, which, as I have gained weight over the years (starting with a 30 lb. weight gain in podiatric medical school) my feet have become increasingly symptomatic with worsening morning talonavicular pain. I won’t go into further detail (that could be its own editorial), but will say this pain has increased in proportion to my weight gain.
Effect on Podiatrists
Obesity may have many direct and indirect diseases associated with it, but for us podiatrists, we get hit with a double whammy. Yes, the prevalence of diabetes, heart disease, and others are increased with obesity. Additionally, though, we have to deal with the direct effects of obesity on our organ of choice: the foot and ankle. Not only do we have to deal with the diabetic with painful peripheral neuropathy and their increased risk of ulceration, infection, and amputation, we also have to combat the direct effects of their greater weight on the foot: collapse of a structure that is simply unable to support the great weight above.
Riddle and colleagues performed a case-control study and found a 5.6 times increased risk of plantar fasciitis in patients with obesity.4 From a purely anecdotal standpoint, I cannot count how many of my symptomatic adult flatfoot patients are overweight. In fact, obesity is a known risk factor for adult acquired flatfoot (posterior tibial tendon dysfunction). Similarly, a majority of the ankle fractures I repair are in obese patients, and when I repair a comminuted ankle fracture, it is mostly likely in an obese patient. So many factors go into making these patients highly complex, be it osteopenia from lack of use, repetitive pressure overload, or systemic diseases.
The challenges to treating the obese patient are many, and medical professionals, be they primary care physicians or specialists, need to do more. What should we do? What can we do? We don’t have the option to just throw up our hands and give up. In part 2 of our miniseries next week, we’ll discuss the tools and research available to help physicians optimize the health of their obese patients.
Until then, I’ll see you at the gym!
Best wishes.

Jarrod Shapiro, DPM
PRESENT Practice Perfect Editor
[email protected]
References:
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. Dietary guidelines for Americans. 6th ed. Washington, DC: U.S. Government Printing Office, 2005.
- Prevalence of Obesity in the United States, 2009-2010. NCHS Data Brief. Jan 2012. 82.
- Obesity Prevalence in 2011 Varies Across States and Regions. https://www.cdc.gov/obesity/data/adult.html
- Riddle D. et al. Risk Factors for Plantar Fasciitis: A Matched Case-Control Study. JBJS, May 2003; 85A; (5): 872-877.
Get a steady stream of all the NEW PRESENT Podiatry
eLearning by becoming our Face book Fan.
Effective eL earning and a Colleague Network await you. |
 |
This ezine was made possible through the support of our sponsors: |
|




















.jpg)











