|
Robert Weinstein, DPM
Ankle & Foot Centers
Atlanta GA |
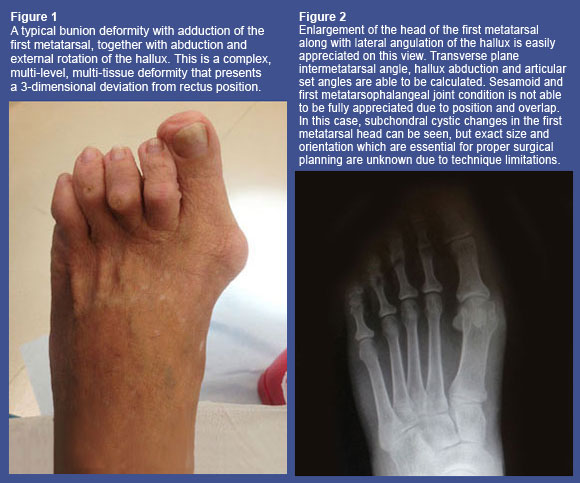
Evaluation of the condition we commonly call a 'bunion' is a rather complex process most podiatric physicians perform routinely. Many patients will present to the clinic with complaints of pain or pressure from "the bump on the inside of my foot." Of course, they will often call it a bump, bunion, or spur, but I have not yet had any patients present themselves complaining of their "hallux abducto-valgus deformity." Yet immediately, as a foot and ankle surgeon, I translate the "bump" into a triplane orthopedic deformity having osseous and soft tissue components and involving four separate bones. Interesting how quickly that happens when you think about it.
In the course of evaluation, clinical aspects such as how large the prominence is, how painful it is to pressure and movement, the tendency to track with range of motion, the extent and quality of motion, the amount of instability at adjacent joints, and secondary anomalies such as sub second metatarsal tyloma are noted. Plain-film radiographs are certainly a routine part of the complete examination, and will include the obligatory 3-projection series: dorsoplantar, medial oblique, and lateral images. From these projections, we define angulational values and make note of other anomalies such as degenerative joint changes, articular flattening, bone stock and width, and any adjacent conditions that may contribute to the deformity or require attention in the course of any corrective procedures.
The dorsoplantar radiograph is used for calculation of the transverse plane angulations: intermetatarsal angle, hallux abduction angle, hallux interphalangeus angle, metatarsal-cuneiform obliquity angle, proximal and distal articular set angles, and sesamoid position. The medial oblique projection may show axial deviations of the first metatarsal from the second metatarsal, but is more informative for evaluation of arthritic changes of the sesamoids. Finally, the lateral projection may also be used to assess metatarsal axis deviation, but is probably best suited to examine the condition of the head of the first metatarsal for flattening or spurring because of the superimposition of the lesser metatarsals.
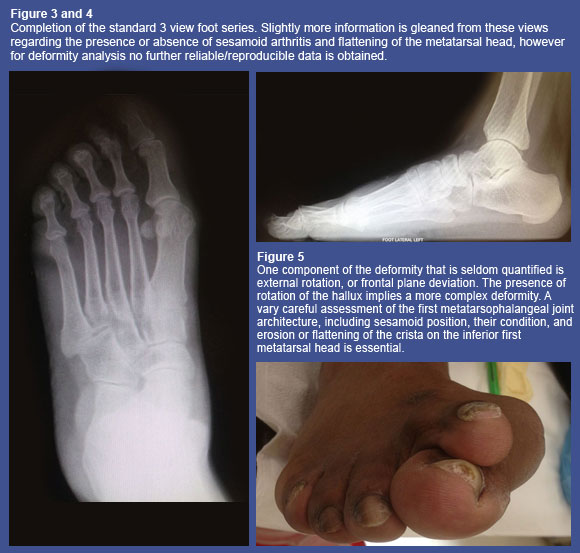
From the 3-projection series, we quantify transverse plane deformity (the 'hallux' and 'abduction' components). What about the frontal plane? Using standard radiographs, there is no analysis or quantification of the frontal plane deformity, the 'valgus' component. We have to mentally 'interpolate' this information, since our standard images cannot adequately capture this plane (credit to Guido Laporta, DPM for the description of this process). Creative positioning, wedges and taping, along with sesamoid axial projections, can show sesamoid deviations, which is a component of the frontal plane deformity, but true deformity analysis should be performed in the patient's normal stance position, not in artificial constructs.
Figure 6
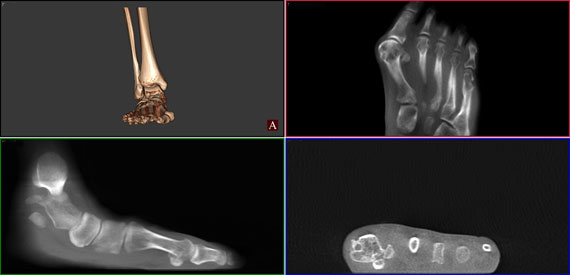
Weight Bearing Cone-Beam CT Bunion Evaluation. This technique couples the reliability of weight bearing 3-dimensional imaging for deformity analysis with the ability to subtract layers for isolated structure assessment. Here different windows show a mild hallux valgus deformity, with larger abduction component on the right foot. The sesamoid-metatarsal articulation is more precisely appreciated, including blunting of the crista. The pedCAT can slice at 0.3mm increments, giving an incredibly detailed image of the first metatarsophalangeal joint complex. |
|
|
Since the condition is a tri-plane (3-dimensional) deformity, then understanding all of the components and their angular values contributing to the deformity would be essential for appropriate description. This is not merely an academic exercise, especially when considering that a large number of these patients go forward with surgical correction. Clearly, better deformity analysis leads to better pre-operative planning, surgical execution, and post-operative results. This is where 360-degree radiography, or computed tomography (CT), excels. Traditional CT evaluation would seem exceptional as a standard tool, given the additional radiation and lack of weight bearing reliability for quantification. However, weight bearing cone-beam CT found in the pedCAT™ (Curvebeam, Philadelphia, PA) eliminates these problems, providing extremely high resolution volumetric (3D) images using approximately the same radiation as a standard plain-film series.
Figure 7
Axial markers and measuring tools easily overlay bone structures and measurements are automatically calculated. Bone lengths, centers of deformity, size and location of defects, and contralateral comparisons are easily obtained. |
|
|
Figure 8
Full view of a severe bunion deformity with volumetric representation. Cyst formation in the metatarsal head is appreciated on the axial view. Coronal section demonstrates near total dislocation of the sesamoid apparatus and complete flattening of the crista, while the metatarsophalangeal articulation is spared. These findings are often obscured or not obtained in plain film series. Without knowing this anatomy in detail, consideration would be given to joint reconstruction procedures (metatarsal osteotomies, Lapidus-type fusion, etc.) However, the likelihood of success of joint salvage in this case is severely limited. |
|
|
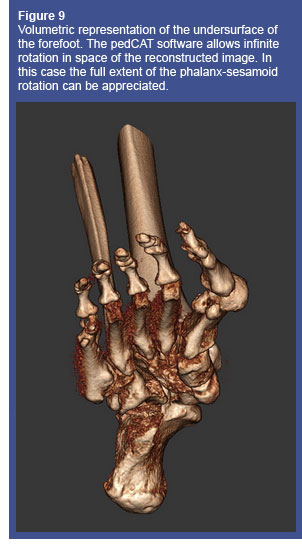 In the pedCAT, the patient stands in their relaxed calcaneal stance position for approximately 60 seconds while the image is taken. After the scan, the computer reconstructs the data gathered from the sensor and within minutes, a full 3D reconstruction of the foot is available to view in the software environment. Contrast enhancement, soft tissue windows, magnification, measuring tools, and cross-sectional or subtractive slicing are all available to more closely look at the deformity. The data can then be exported into EMR software to attach to a patient's file, uploaded in PACS or DICOM format to an off-site radiologist, or printed onto a CD with a software viewer package, to view on another computer.
In the pedCAT, the patient stands in their relaxed calcaneal stance position for approximately 60 seconds while the image is taken. After the scan, the computer reconstructs the data gathered from the sensor and within minutes, a full 3D reconstruction of the foot is available to view in the software environment. Contrast enhancement, soft tissue windows, magnification, measuring tools, and cross-sectional or subtractive slicing are all available to more closely look at the deformity. The data can then be exported into EMR software to attach to a patient's file, uploaded in PACS or DICOM format to an off-site radiologist, or printed onto a CD with a software viewer package, to view on another computer.
The concept of 'deformity evaluation' should not be considered as the territory of only the most advanced reconstructive surgeons. Most podiatric physicians, in one capacity or another, perform this activity daily, whether in a formal, quantitative manner or more qualitatively in the clinic. In addition to bunions and first ray pathology, pes valgus, cavus foot and its variants, second toe pathology, fractures, and Charcot joints are all three-dimensional conditions that are commonly encountered and evaluated. The pedCAT provides a tool to make accurate, quantitative assessment in the weight-bearing state of these and many more conditions.
Since there is an expansion of physicians treating foot and ankle disorders in much more complicated ways, a variety of tools are coming to market to allow for more exact analyses. As with any scientific advancement, there is an expectation that measurement and precision are part of this transformation. Evaluation and measurement of deformity in three dimensions rather than two completes the quantitative picture, taking precision and decision making to the next level.


The pedCAT™, first in-office TRUE 3D weight-bearing CBCT device for the foot and ankle, puts optimal treatment planning at your fingertips for greater confidence of increased predictability in surgical outcomes. With virtually the same radiation dose as that of traditional 2D X-rays and 99% less radiation of a traditional medical CT scan, the pedCAT™ assesses clinical conditions including, but not limited to, fractures, dislocations, arthritic joints, and early detection of osteomyelitis for quicker diagnosis, evaluation and treatment planning. |
|
For more information or to request an in office demo of the pedCAT,
please contact us at 866.400.0035 or [email protected]. |