|
Alex Tievsky, DPM
Tievsky Foot & Ankle PLLC
New York, NY |
A patient presents with pain at 1st metatarsal on initial visit, and the pain travels up to his lateral ankle on the third follow up. This is obviously an exaggerated scenario, but we see patients with vague bony pain all too often in our practice. Does this mean that our patients are doomed to suffer countless different foot problems? Or does it simply mean that a large chunk of our patients are crazy and can't make up their mind on what hurts? While the latter point is debatable, in most instances a patient’s "real" problem will cause the patient to feel pain in MORE than one location.
Referred pain is nothing new in the art of diagnosing and treating a weight bearing part of the human body. Our body constantly corrects and adjusts itself with the intent to fix any pathology that plagues it, thereby complicating the diagnosis of the origin of this pain. The real question becomes, how do we effectively diagnose a patient whose pain is referred? While the vast majority of us use our physical and gait exams to get down to the root of the problem, it may still not be enough to get the correct diagnosis in a timely manner.
Many physicians have joined 20th century medicine and utilize tests such as ultrasound, X-ray, CT scans, MRI, etc. We see the benefit of these tests, and yet there is usually a delay between when the patient was given a referral to get these tests and when treatment really begins. The delayed treatment gap has compelled a lot of practitioners to get an X-ray or ultrasound machine in their office. If you ask any one of them if they can effectively practice without these tests, they will most likely shout NO! Having the luxury to diagnose complicated foot problems with same day diagnostic exams means patients spend less time in pain and have a quicker recovery.

I am proud to present you with a great new diagnostic tool to bring you into the 21st century. The pedCATTM is a weight bearing 3D CT scan device for your office. Unlike traditional X-rays, it shows you a three-dimensional slice by slice view, as well as a reconstructed 3D view, that you could otherwise only get from a hospital CT scan. Moreover, the patient can be scanned fully weight bearing, and the device doesn't emit anywhere near the radiation produced by one conventional CT scan. The pedCAT takes away any guesswork from reading conventional two-dimensional X-rays and you can print out or input any views into your Electronic Medical Record (EMR). Another benefit is that you can send any of the scans directly to a radiologist and they will provide a reading for the CT scan that will automatically be updated on your own EMR. There are countless financial benefits to using a pedCAT in your office that Dr. Stanley Kalish touched on in his review of this great diagnostic tool. (click here for article)
However let me stop talking about all the many reasons why I love using an in-office weight bearing CT scanner and give you an example of how it recently helped me make a diagnosis that would probably have been missed otherwise.
CASE PRESENTATION
A 38-year-old female presented to my office with pain in her right foot and chronic pain in the lower calf area. She had right calf pain on and off since she was a teenager and did not recall any trauma to the area. She was not a smoker, had not traveled on an airplane lately, and was not on birth control pills. Her dorsal forefoot was painful and edematous on palpation and the 2nd MPJ was the area of maximum tenderness. She denied any trauma or any other medical problems. In fact, she had never visited a doctor before in her native country of Syria.
 Items on the differential diagnosis list include most notably, DVT, stress fracture, rheumatoid arthritis, phlebitis and many more. The list is long, given all the vague history and generalized pain on physical exam. Before I sent the patient for vascular tests to rule out a DVT, I wanted to see what the foot/leg looked like on X-ray/CT. A pedCAT scan was performed in office and one minute later we had our “mystery diagnosis”.
Items on the differential diagnosis list include most notably, DVT, stress fracture, rheumatoid arthritis, phlebitis and many more. The list is long, given all the vague history and generalized pain on physical exam. Before I sent the patient for vascular tests to rule out a DVT, I wanted to see what the foot/leg looked like on X-ray/CT. A pedCAT scan was performed in office and one minute later we had our “mystery diagnosis”.
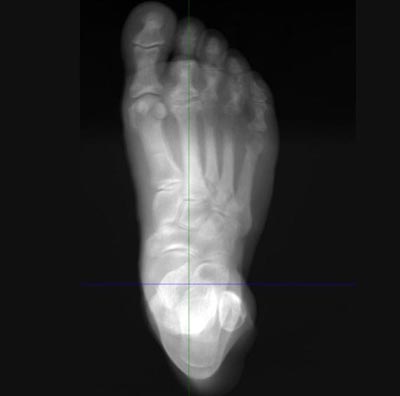
As you can see in Figure 1, she has a large calcification on her 2nd MPJ neck dorsally. The lesion extends all the way up to the dermis.
Figure 1
An abnormal exostosis is seen forming from the 2nd MPJ area. The consistency of it is not fully bone but is closer to calcified soft tissue. The bullet is also seen next to the fibula. |
|
|
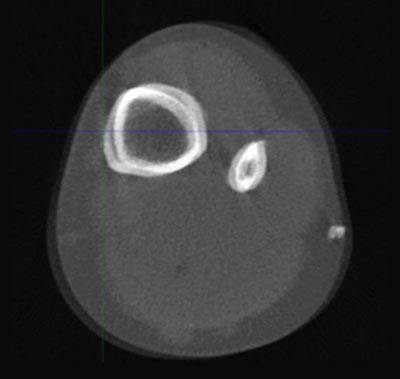
Because of the way the lesion spreads into the dermis (see Figure 2), the only real possibility was a rheumatoid nodule.
Figure 2
The exostosis above the 2nd MPJ does not have a clear dorsal cortex and soft tissue surrounding it are cloudy and irregular. |
|
|
The patient was sent for blood work right after the visit and rheumatoid arthritis (RA) was confirmed. As for the leg, if you look at the posterio-lateral aspect of her fibula (Figure 3), you can see a metallic object which, when zoomed in, was deemed to be a bullet. The patient denied getting shot but stated it was possible, because soldiers forced her family out of her home when she was a teenager and started firing at the floor to get them out faster. Her lower extremity area showed no signs of a scar from a bullet wound, but given the pedCAT readings, we continued our evaluation and a scar was found on the patient’s thigh. This correlated with the scenario of her getting shot.
Figure 3
The remainder of what appears to be a bullet is found posterior and laterally to the fibula. |
|
|
From this one sub-minute exam, we were able to deduce two complex diagnoses which would have, no doubt, taken a lot longer to find and treat if we only had a plain X-ray exam available. Plain films (X-rays) are an old technology that have not changed since its discovery in 1895, and while we have made many advancements in ways to view the X-ray (digital), we are still left with a substandard two-dimensional view of a three-dimensional problem. Diagnosing RA without a strong family history or previous blood work can be a tricky business. While we can easily diagnose late stage RA with joint erosions and lateral digit deviation, the more common earlier stages of RA often get missed with few clues given on plain films.
The rheumatoid nodule and bullet were both evaluated and a surgical plan was deduced on the first visit. I am constantly impressed with the clarity of pedCAT exams and would strongly urge every serious foot and ankle surgeon to consider utilizing this device. It will help your patients and your practice, and will give you a huge edge over your competitors both financially and by word of mouth. Podiatrists from the surrounding area routinely ask to scan patients on my pedCAT machine to save time with a quick diagnosis. On a side note, ever since getting the pedCAT, I have sold my X-ray machine and use the pedCAT both for X-ray views and CT scans. In my opinion, this is a device you will use repeatedly every day. It is a great investment that will pay for itself.
For all of my fellow peers just coming out of residency, it is important that you start practicing current medicine and use your new found training with the best tools at your disposal. The way podiatry was practiced 50 years ago was different from the way it was practiced 20 years ago, is different today, and will no doubt be different in the way it will be practiced in 20 years from now. If you stay current with your diagnostic and treatment protocols, you will always stay within the accepted standard of care and will be more capable of helping your patients and staying ahead of the competition. The key to success is learning from your teachers, but also to add your own current knowledge to the way you practice. At the end of the day, this particular technology will help you every day of your career.

The pedCAT™, first in-office TRUE 3D weight-bearing CBCT device for the foot and ankle, puts optimal treatment planning at your fingertips for greater confidence of increased predictability in surgical outcomes. With virtually the same radiation dose as that of traditional 2D X-rays and 99% less radiation of a traditional medical CT scan, the pedCAT™ assesses clinical conditions including, but not limited to, fractures, dislocations, arthritic joints, and early detection of osteomyelitis for quicker diagnosis, evaluation and treatment planning. |
|
For more information or to request an in office demo of the pedCAT,
please contact us at 866.400.0035 or [email protected]. |