|
|
|
|
Pre- or Post-op?
When is the Best Time to Inject?
Part Two: Clinical Questions
|
|
|
|
|
|
|
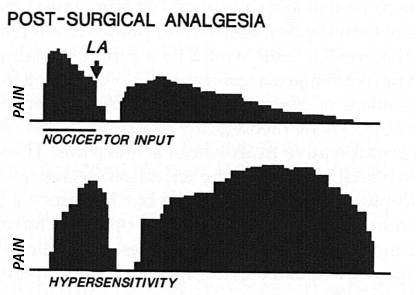
The basic science has shown us rather clearly that preemptive analgesia is a highly important method to help us control postoperative pain. In last week’s issue, we identified the mechanisms of peripheral and central sensitization and their roles in postoperative pain. As a quick illustration, take a look at the following images taken from Woolf and Chong’s excellent review1.
|
|
|
This first image shows what occurs when the analgesia occurs after the surgical incision. You’ll note that the local anesthetic (LA) is given at the end of the surgery (indicated by the bar under the “nociceptor input” graph). Notice the return of pain, which diminishes over time, but also the significant hypersensitivity of the patient’s nervous system.
|
|
|
|
|
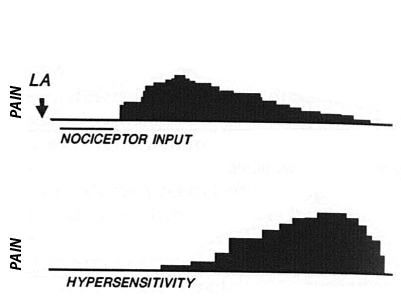
Take a look, now, at the graph where local anesthetic is given before the surgery. The initial surgical pain is avoided, and the postsurgical pain resolves over time, but the hypersensitivity is also significantly diminished. This is the benefit of single modality pre-emptive analgesia.
|
|
|
|
|
|
|
|
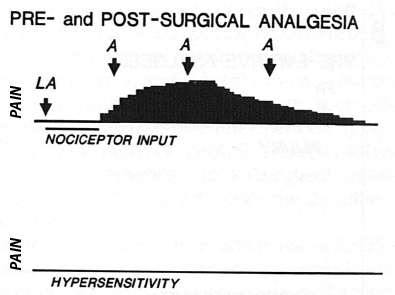
The third graph adds another level to our discussion, which brings us to the ideas of pre- and postoperative analgesia and multimodal analgesia. You’ll note on the graph that giving an injection before the surgery but also maintaining that analgesia during the postoperative period eliminates the central and peripheral stimulation associated with greater postoperative pain.
|
|
|
|
|
With the basic scientific rationale established, a few questions come up, including: what methods exist to help us create effective pre-emptive analgesia? What does the clinical evidence show? Is a single treatment method such as local injection enough or should we combine methods for greater effect? Let’s discuss these issues and see if we can hone our preemptive methods a little further.
|
|
|
Methods to Establish Pre-emptive Analgesia and the Evidence

|
|
|
There are actually several reasonable modalities to help physicians decrease their patients’ postoperative pain. We’ve already discussed the popliteal block in Practice Perfect 540, entitled, “POP Goes the Block”. This regional block, done before the incision, breaks the connection between the limb and the central nervous system, reducing the risk of both peripheral and central sensitization. However, this method does not stop the delayed postoperative inflammation that may cause later hypersensitivity unless one considers the use of in-dwelling catheterization, maintaining anesthesia for up to three days. Similarly, local anesthesia about the foot and ankle before incision is also beneficial as a pre-emptive analgesic technique. This method has been well-used in the podiatric community.
|
|
|
It’s important to understand that spinal or epidural anesthesia should not be used for this purpose because these methods do not stop the central sensitization that may occur1.
|
|
|
Migues et al compared the popliteal block to local foot blocks (both done using nerve stimulation and ultrasound) and found a 96% satisfaction rate for both with a four-hour longer anesthesia time with the popliteal block (14 hours) and just over 40% of patients being pain-free by visual analogue scale (VAS) at 24 hours2.
|
|
|
|
|
Gadek and colleagues also found local foot blocks to be highly effective in a prospective study of 118 patients undergoing distal metatarsal osteotomy bunionectomy and randomized to either spinal anesthesia plus pre-emptive local block or spinal anesthesia plus saline placebo. At 24 hours postop, the placebo group had a VAS of 3.0 versus 1.3 in the preemptive group. The placebo group had a 42.4% need for rescue medication versus 11.9% in the preemptive group3. These statistically and clinically significant differences demonstrate the effect of pre-emptive analgesia in forefoot surgery.
|
|
|
Other methods of pre-emptive analgesia include opioids given during anesthesia induction (preventing depolarization in dorsal horn neurons leading to the prevention of central sensitization), NSAIDS, neurologically active medications and combinations of the above.
|
|
|
For example, Montazeri and partners found a preoperative oral 300 mg gabapentin dose to be significantly beneficial in reducing 24 hour postoperative pain and morphine use in 70 patients undergoing lower extremity orthopedic surgery4. Sebastian and colleagues found similar results with 150 mg pregabalin in 90 randomly assigned patients5.
|
|
|
|
|
It should be noted that there are some contradictory results with the use of pre-emptive analgesic methods, but it is hard to judge due to the heterogeneity of methodology. Additionally, some of these contradictory studies have methodological flaws that weaken their predictability. For example, Khahi and associates did not find oral gabapentin to help with postoperative pain6, but their study looked at the administration of this medication after surgery rather than before. Considering the physiology of peripheral and central sensitization, it is not surprising they obtained this result.
|
|
|
On balance, it appears the research supports the physiology and urges us to adopt pre-emptive analgesia as the method of choice to best help with postoperative pain reduction.
|
|

-
Woolf CJ, Chong MS, Preemptive Analgesia – Treating Postoperative Pain by Preventing the Establishment of Central Sensitization. Anesh Analg. 1993 Aug;77(2):362–379.
Follow this link
-
Migues A, Slullitel G, Vescovo A, et al. Peripheral foot blockade versus popliteal fossa nerve block: a prospective randomized trial in 51 patients. J Foot Ankle Surg. 2005 Sep-Oct;44(5):354-357.
Follow this link
-
Gadek A, Liszka H, Wordliczek J. Postoperative pain and preemptive local anesthetic infiltration in hallux valgus surgery. Foot Ankle Int. 2015 Mar;36(3):277-281.
Follow this link
-
Montazeri M, Kashefi P, Honarmand A. Pre-emptive gabapentin significantly reduces postoperative pain and morphine demand following lower extremity orthopedic surgery. Singapore Med J. 2007 Aug;48(8):748-751.
Follow this link
-
Sebastian B, Talikoti AT, Nelamangala K, Krishnamurthy D. Effect of Oral Pregabalin as Preemptive Analgesic in Patients Undergoing Lower Limb Orthopedic Surgeries Under Spinal Anesthesia. J Clin Diagn Res. 2016 Jul;10(7):1-4.
Follow this link
-
Khahi MP, Marashi S, Khajavi MR, et al. Postoperative Gabapentin to Prevent Postoperative Pain: A Randomized Clinical Trial. Anesth Pain Med. 2012 Autumn;2(2):77-80.
Follow this link
|
|
Get a steady stream of all the NEW PRESENT Podiatry eLearning by
becoming our Facebook Fan.
Effective eLearning and a Colleague Network await you.
|
|
Grand Sponsor
Major Sponsor
|
|