INTRODUCTION
In this discussion on subchondral fractures of the metatarsal head, we thought it prudent to start with a short synopsis of stress fractures. First described by Aristotle in 200BC, stress fractures are any fracture or micro-fracture caused by a repetitive loading on bone, rather than a single traumatic event (1). Stress fractures occur in a number of patient populations, including elite and recreational athletes, the general population and those suffering from systemic disease. Stress fractures are more common in females than males (5:1)(2) and those active in sports (1).
Stress Fractures can broadly be divided into two etiological categories: Insufficiency Fractures (those caused by normal stresses on abnormal bone) and Fatigue Fractures (those caused by abnormal stresses on normal bone). Gehrmann and Renard (1) further divide the etiological causes of stress fractures into Intrinsic and Extrinsic factors, listing excessively high arches, leg-length discrepancies, bone density or hormonal factors as Intrinsic factors and training regimen, equipment and nutrition as components of extrinsic factors. In a study by Matheson et al. (3) who looked at 320 athletes that presented with stress fractures, they reported stress fractures to occur most often in the tibia (49.1%), followed by the tarsal bones (25.3%) and the metatarsals (8.8%). They further noted that patients who were runners, were more likely to develop stress fractures and further noted that only 9.8% of those that had x-rays done upon initial presentation displayed radiographic evidence of a stress fracture. The low incidence of stress fractures that display radiographic evidence on initial presentation make it important that the physician be aware of the possibility of a stress fracture, especially subchondral metatarsal head stress fractures.
SUBCHONDRAL METATARSAL HEAD STRESS FRACTURES
The literature is amass with information regarding subchondral stress fractures of the femoral head (4,5), but the same cannot be said for subchondral stress fractures of the metatarsal head (6,15). The similarity of the presenting symptoms in subchondral fatigue fractures and that of other, more commonly seen conditions such as: metatarsalgia, tendonitis, capsulitis, pre-dislocation syndrome, neuroma and stress fractures of the metatarsal neck, makes early diagnosis difficult. There are however, numerous articles on Juvenile Freiberg’s infraction, first described by Freiberg in 1914. In his original article he attributed the cause of second metatarsal head collapse (infraction), to trauma and disruption of the subchondral blood supply caused by increased length of the second metatarsal leading to a increase in plantar pressure under the metatarsal head (12). In discussions on work done by Freiberg and Kohler, a number of authors have proposed the possibility of a multifactorial etiology in the development of Freiberg’s Infraction, combination of vascular insult, repetitive micro trauma, systemic disease and biomechanical malalignment (6,12). Freiberg’s infraction is generally regarded as a condition seen in young females, but has been reported in ages 17-77 (12). It is suggested that Freiberg’s presents in younger age groups due to vulnerability and disruption of the epiphysis during osseous maturation (3).
There is limited information regarding development of Freiberg’s in the non-juvenile patient. Subchondral metatarsal head fractures and Non-juvenile Freiberg’s Infraction, occur in distinct age groups but share radiographic and pathophysiological similarities (8). Gauthier and Elbaz (16) suggest that subchondral fatigue fractures are part of the pathologic development of Non-juvenile Freiberg’s Infraction. These two conditions may be confused with gout, neuroma or second ray syndrome (7). A study by Young et al. (8), suggest that Non-juvenile Freiberg’s Infraction of the metatarsal head is due to “shearing osteochondral disruption” at the mineralized and non-mineralized bone interface “tide-water mark” and not a true avascular necrosis of the metatarsal head. Young et al. (17) suggests that during toe-off when the proximal phalanx is held in a fixed position by the ground reaction force, two moments are created: one parallel to the “tidewater mark” and the other perpendicular to the articulation of the MTPJ. As the proximal phalanx is firmly compressed into the dorsal aspect of the metatarsal head during toe-off, shearing stresses parallel to the subchondral bone interface act upon the metatarsal causing it to sheer plantarly, leading to disruption at the metatarsal head and possible Non-juvenile Freiberg’s Infraction (17). A study by Lee and Donatto (9) suggests that during running the highest bending and shearing forces develop within the second metatarsal, supporting work by Young et al. (17).
Athletes engaged in repetitive activity with recent increases in training or competition are at risk for stress fractures of the foot and ankle. Physical and radiographic findings are often unremarkable and diagnosis may be difficult. Although many of these injuries may be managed symptomatically, certain types of stress fractures are at higher risk for delayed union, nonunion, or re-fracture without aggressive immobilization or surgical fixation(10). Smith and Kreibich(11) note that according to Hoskinson the most reliable view on x-ray for detection of an early lesion is a 45° oblique of the forefoot.
Lechevalier et al (8) noted consistently favorable outcomes on x-ray over a one month period of non-weight-bearing, for 11 patients treated.
The purpose of this article is to reinforce the astute clinicians awareness of this often missed diagnosis, and in so doing enable the physician to make the diagnosis earlier and possibly avoid long term sequela by earlier more aggressive management. Future study with regards to early detection and intervention in subchondral metatarsal head stress fractures is needed. We present the following 2 cases along with a comparison and final sequela at the end:
CASE REPORT 1
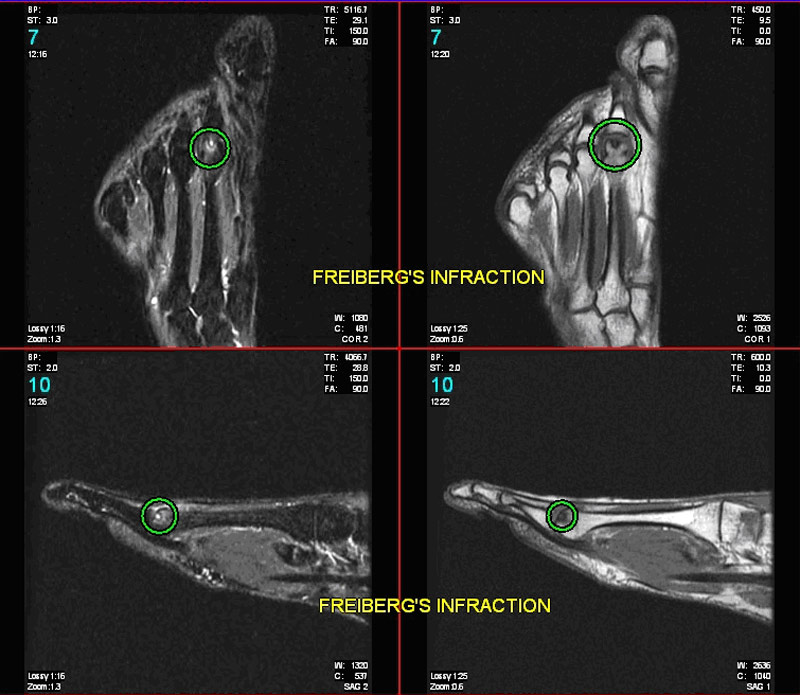
The patient is a 42 year old female who presented to a podiatrist for removal of painful internal hardware of the left first metatarsal. The patient had a secondary complaint of pain in the second metatarsal of the opposite foot for almost 1 year with gradual increasing intensity over the past three to four months. She experienced an increase in pain on ambulation in flat and high heeled shoes and remarked that the pain radiates, at times along her second toe. She could recall no history of trauma and had not sought any previous treatment. X rays were reportedly negative for bony pathology. She was referred to our office for a diagnostic Ultrasound to rule out a neuroma. A Diagnostic Ultrasound did not show any Hypo-echoic lesions within the second interspace of the right foot, indicating the unlikely presence of an interdigital neuroma. An area of Hypo-echoic signal was, however noted around the second MTPJ, this appeared to be within the capsule. A plantar plate tear was not noted however a small metatarsal head fracture was also noted at the surface of the second metatarsal head. Clinical exam revealed acute pain on palpation of the second metatarsal head/neck region. Xrays were taken and revealed a lucency in the second metatarsal head (Figure 1). There was no visible collapse of the subchondral bone or callus formation in the region of the head or neck. A preliminary diagnosis of subchondral stress fracture of the metatarsal head with early secondary Freiberg’s infarction was made. The patient was placed in a cam walker, instructed to be non-weight bearing and referred for an MRI. The MRI revealed a well circumscribed cystic lesion within the dorsal aspect of the second metatarsal head with surrounding marrow edema. The patient eventually required surgery on the second MPJ which included a Weil Osteotomy which resolved her complaint.
|
Figure 1: suspicious lesion in subchondral bone of 2nd metatarsal head.
|
| Click on the image below for a larger view. |
|
Figure 2: marrow edema noted in subchondral bone of 2nd metatarsal head. |
CASE REPORT 2:
A 62 year old female presented to our office with a chief complaint of a painful left foot. The pain had been present for three weeks and had been increasing in severity during the past week. The patient had been running three miles per day five to six times per week in addition to participating in other sports. On examination the second MTPJ and digit appeared edematous with pain on palpation of the second digit and second metatarsal head and neck from the dorsum. There was also pain on palpation of the 2nd MTPJ dorsally and plantarly. There was no pain on palpation of either the second or third digits. The differential diagnosis included stress fracture of the second metatarsal neck, stress fracture of the 2nd met head, pre-dislocation syndrome and plantar plate tear. The patients past medical history was unremarkable.
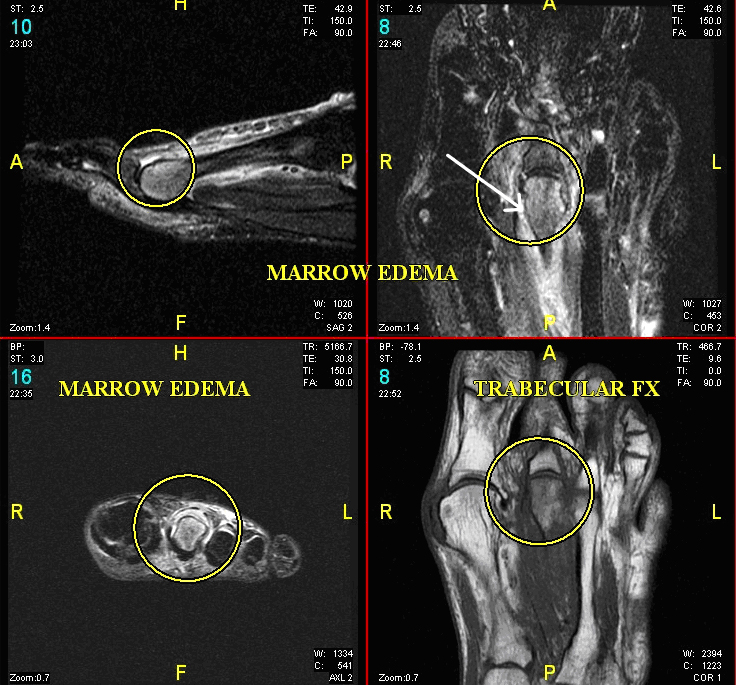
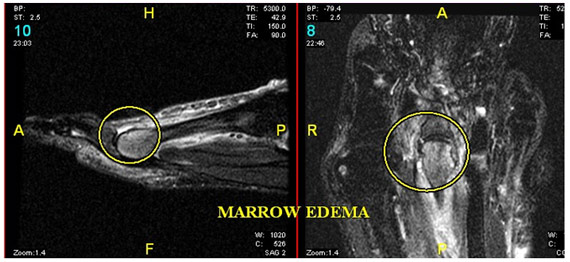
X-rays (figure 3 below) of the left foot showed no visible signs of fracture, although some questionable irregularity was noted at the cartilaginous surface of the second metatarsal head. An MRI taken the same day (figure 4) showed marked marrow edema within the distal one third of the second metatarsal with concomitant linear hypointense areas within the metatarsal head consistent with a nondisplaced fracture. A diagnosis of subchondral stress fracture of the second metatarsal head was made. There were no abnormal findings of the metatarsal neck or plantar plate. The patient was treated with non weight bearing, a cam walker and a bone stimulator.
|
Figure 3: Irregular joint surface |
Click on the image below for a larger view. |
|
Figure 4: Increase in marrow edema in head of 2nd metatarsal |
|
Figure 5a shows an MRI of a classic stress fracture of the metatarsal neck. |
|
Figure 5b shows a stress fracture of the metatarsal head. The MRI is useful in differentiating metatarsal neck vs metatarsal head stress fractures. |
The x-ray show below are of a ballet dancer, 75 years old with no history of musculoskeletal disease who is still dancing. His x-rays show what may have been multiple episodes of Non-juvenile Freibergs Disease. He has a history of multiple foot injuries during his career. The patient had surgery on the left first and fifth metatarsals only. All of the rest are presumably Non-Juvenile Freiberg’s disease. |
|
Dr. Meisler would like to acknowledge 20/20 Imaging for providing the digital x-ray images and East River Imaging for helping with the MRI images. |
References:
-
Gehrmann R. M, Regis L, Renard M. D, Current Concepts Review: Stress Fractures of the Foot, Foot & Ankle Int. 2006 Sept., 27(9), 750-57.
-
Botek G, Anderson M. A, Balis G, Dorsiflexory Wedge Osteotomy to Treat Freiberg’s Infraction of the Second Metatarsal Head: A Case Report, Podiatry Internet Journal, Sept 2007, 2(9):1
-
Carmont, MR; Rees, RJ; Blundell, CM: Current Concepts Review: Freiberg’s Disease. Foot & Ank. Int. 10(2): 167-176, 2009
-
Freeman M.A.R, Day W.H, Swanson S.A.V. Fatigue Fracture in the Subchondral Bone of the Human Cadaver Femoral Head, Med. & biol. Engng. Nov 1971, 9(6):619-629.
-
Davies M, Cassar-Pullicino VN, Darby AJ. Subchondral insufficiency fractures of the femoral head, Eur Radiol. 2004 Feb;14(2):201-7.
-
Brukner P, Bennell K, Stress fractures in female athletes. Diagnosis, management and rehabilitation, Sports Med 1997, Dec, 24(6): 419-29.
-
Torriani M, Thomas B.J, Bredella M.A, Ouellette H, MRI of Metatarsal Head Subchondral Fractures, AJR. March 2008, 190(3):570-575.
-
Lechevalier D, Frounier B, Leleu T, Crozes P, Magnin J, Eulry F Stress fractures of the heads of the metatarsals. A new cause of metatarsal pain, Rev Rhum Engl Ed., 1995 April, 62(4):255-9.
-
Lee, EW; Donatto, KC: Fractures of the midfoot and forefoot. Curr. Opin. Orthop. 10:224-230, 1999.
-
Chen R.C, Shia D.S, Kamath G.V, Thomas A.B, Wright R.W, Troublesome stress fracture of the Foot and Ankle, Sports Med Arthrosc. 2006 Dec, 14(4):246-51.
-
Smith T.W.D, Kreibich D.N, Freiberg’s Disease In Hallux Valgus and forefoot surgery, Hetherington, VJ (Ed), Churchill Livingstone, New York 1988. p.453-457.
-
Tsujii M, Hasegawa M, Hirata H, Uchida A: Subchondral insufficiency fracture of the second metatatarsal head in an elderly woman treated with autologous osteochondral transplantation, Arch Orthop Trauma Surg. 2008 Jul, 128(7): 689-93.
-
Petrisor B. A, Ekrol I, Court-Brown C, The Epidemiology of Metatarsal Fractures, Foot & Ankle Int., March 2006, 27(3):172-174.
-
Chowchuen P, Resnick D: Stress fractures of the metatarsal heads, Skeletal Radiol, 1998 Jan, 27(1): 22-5.
-
Chuckpaiwong B, Cook C, Pietrobon R, Nunley JA: Second metatarsal stress fracture in sport: comparative risk factors between proximal and non-proximal locations, Br J Sports Med. 2007, Aug, 41(8):510-4.
-
Gauthier G, Elbaz R, Freiberg's infraction: a subchondral bone fatigue fracture. A new surgical treatment, Clin Orthop Relat Res. 1979, Jul-Aug (142): 93-5.
-
Young M.C, Fornasier V. L, Cameron H. U, Osteochondral disruption of the second metatarsal: a variant of Freiberg’s infraction?, Foot & Ankle Oct 1987, 8(2):103-9.
|
|