Current Mainstream Podiatric Biomechanics
Part II: The Foot Centering Theory
|
By Dennis Shavelson, DPM
Biomechanics Editor, PRESENT Podiatry |
When listening to Dr. Ed Glaser discuss MASS Theory, it is hard to argue that in closed chain, the foot is more efficient, better able to counter the effects of gravity and underlying biomechanical pathology and the bioengineering of our sedentary lifestyles, when optimal functional position and balance are maintained.
Likewise it is hard to refute Dr. Kirby’s SALRE argument that reducing the forces causing tissue damage to a level below when damage occurs should be part of the targeted plan of practitioners of biomechanics.
Unfortunately, these guru’s of biomechanics, because of financial interests, bias and the lack of evidence proving their theories, have developed their own closed circled followings and rarely incorporate or corroborate the work of others. To quote Yogi Berra “In theory, there is no difference between theory and practice. In practice, there is.”
The Foot Centering Theory - Shavelson
The Foot Centering Theory, originated by this author, rethinks the foundations for diagnosis and treatment of the foot and posture in closed chain professionally with a high goal set in mind. That goal is enabling practitioners to quantify postural deviations and the locations and levels of tissue weakness using Architecture in addition to Engineering and Newtonian Law, in order to create a language for biomechanics that all can understand and discuss.
The theory begins with the fact that an architectural arch has two equal sides or pillars and a central keystone that supports it. The only function of this arch is to support. However, in an engineering sense, when we construct an arch shape using the centering method whose purpose is to move or complete tasks using muscle engine leverage and mechanical advantage, it fails to perform efficiently due to its symmetrical design.
The Foot Arch is Off Centered and Non-Symmetrical
Pedal arches differ from architectural arches, because their bones are inherently off centered and lack balance and equilibrium. The ligaments and muscles lack the strength, leverage and mechanical advantage on one or more of the three body planes to successfully serve as a tie beam for the osseous truss system they bind. Some feet are off centered in the rearfoot, some in the forefoot and some in none or both, and feet even differ within their subgroups.
Every foot has two longitudinal arches connected by a transverse roof, forming an off centered Vault with the back (rearfoot) shorter than the front (forefoot) and the keystone off centered backwards (proximally). Consequently, although some feet are strong and efficient and capable of performing over a lifetime, many feet, foot type-specific, need additional support and training in order to avoid pain and overuse syndromes, injury and deformity over a lifetime.
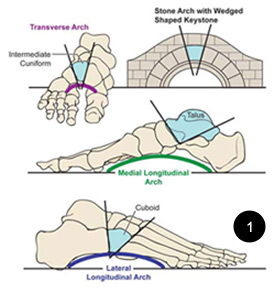
Summarily, pedal arches differ from architectural arches because they are off centered instead of symmetrical (figure 1. below, The Off Centered Arches Of The Foot) . The supporting and driving ligaments and muscles lack the strength, leverage and mechanical advantage to preserve the structure and function of the arches they support and power over a lifetime. They need additional centering support and muscle engine training to get them to support efficiently as though centered.
When scrutinized, some feet are off centered in the rearfoot, some in the forefoot and some in none or both and feet and even feet within these initial subgroups differ in their centering.
The Foot Centering Theory examination profiles all feet into Functional Foot Types®, which can then be examined and treated as subgroups,
initially eliminating many of the variables that reduce the development
of evidence and standards of custom care when feet are examined and
treated as a whole. It looks to prevent and reverse pedal collapse and
loss of muscle engine leverage and mechanical advantage with a
Centering Footbed that incorporates Orthotic reactive Forces in the
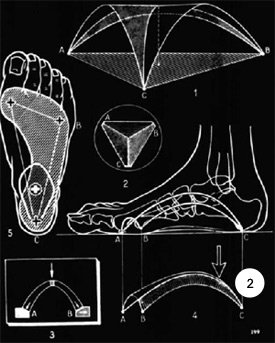
form of shell profile and contour modifications and custom prescribed additions and modifications to the shell. This Foot Centering Orthotic braces the foot in a more “Optimal Functional Position” (figure 2. Above, The Vaulted Foot Is Centered with a Centering Orthotic) where OFP is an approachable imaginary position that exists for each foot, that when assumed, produces the least amount of tissue stress in closed chain function and at the same time maximizes efficient performance of the muscle engines as stabilizers and force units. OFP as in MASS Theory counters pathological forces and improves the leverage of the muscle engines and ligaments, making them more powerful, efficient and trainable.
To this centered shell, orthotic reactive forces (ORF’s) can be added, foot type-specific that when coupled with training of the muscle engines (figure 3. The Muscle Engines Of The Foot) using manual therapy, motor control and manipulations allow practitioners of biomechanics to provide individual patients custom biomechanical care on an interpersonal level until more applicable evidence surfaces.
Instead of “pathology and pain dependent” biomechanics, which is the current standard, Foot Centering is an Integrative Biomechanical Model that leads to a more balanced, efficient, long and productive lifestyle in addition to treating pain and injury.
Makes Explanation of Biomechanics Easier
The Foot Centering architectural language makes presentation, education and marketing of biomechanics easier. It uses independent examination of the rearfoot and forefoot in order to determine deviations from OFP, and it profiles all feet into Functional Foot Types® that can then be treated and researched as independent subgroups.
During The Functional Foot Typing® (FFT) Exam, two separate rearfoot and forefoot tests are taken (RF SERM-PERM, FF SERM-PERM) that classify every foot Functional Foot Types (FFT’s). Each FFT has characteristic weaknesses, strengths, breakdown tendencies and subsequent primary rules for care.
Furthermore, when the amount of motion between the Supinatory End Range of Motion (SERM) and Pronatory End Range of Motion (PERM) …insert link to previous installment that describes these tests…. Tests is determined secondarily, it gives a direction as to how much and what kind of correction best suits the needs of the patient. This SERM-PERM Interval allows practitioners to set approachable high goals for care by countering the many variables previously discussed.
With Foot Centering, care can be applied before, during or after the PIT is reached. This means that it offers preventive and performance enhancement care, reversal of deformity, improved motor control and improved quality of life and not just treatment of pain and injury thereby expanding the scope of biomechanics.
By exposing segmental weakness and collapse in feet, Foot Centering leads to the establishment of primary negative casting rules, foot type-specific that can then be secondarily modified using the SERM-PERM Interval and open and closed chain examination in EBP on a case to case basis, applying casting, prescribing and fabrication techniques that consider OFP and the need for pronatory and supinatory moment counter forces on a case to case basis, supplemented by the training of the muscle engines as needed. In addition, reduction of the impact of variables in this paradigm of care will improve the level and importance of the biomechanical evidence when Foot Centering standards of care are applied.
This introduces the main advantage The Foot Centering Theory has over the other biomechanics paradigms. It is the only paradigm pending patent with The U.S. Patent Agency. This means that using patent protection, both practitioners and laboratories can be held to strict standards if they choose to work with the Functional Foot Typing® method and the Foot Centering Orthotics® and Muscle Engine Training they spawn. This eliminates less qualified practitioners and labs from dilution, unprofessional use or unacceptable fabrication habits for twenty years as the science can grow.
The Foot Centering Model shares aspects with the Root, SALRE, MASS and Sagittal Block theories but they are applied holistically to subgroups of feet instead of treating all feet in reductionist fashion. Human feet, their problems and the physical laws that govern biomechanics has produced many paradigms for care, and none of them, no matter how strongly they claim the opposite, have yet to be inductively tested either with outcome studies or kinematic / kinetic trials with evidence strong enough to be called proven.
Summarily, Foot Centering presents a logical and coherent argument in understandable language when teaching, presenting, documenting and marketing biomechanics to students, practitioners, the foot suffering public and the medical community. It can be considered for use by mainstream biomechanists to lead Podiatry back to its rightful position atop the Biomechanical Pyramid as “The Closed Chain Specialist” that Dr. Root gifted us as thirty years ago.
|














.jpg)


















