Children’s Shoes: A Position Paper
By Dennis Shavelson, DPM
Biomechanics Editor, PRESENT Podiatry
|
|
| |
As a Board Certified Foot and Ankle Surgeon and a Podiatrist that has maintained a biomechanical core and focus on my practice, teaching and mentoring, I have studied and published on the subject of the biomechanics of weightbearing feet and postures from babies to adult, for close to forty years.
Players in the children’s shoe marketplace as well as the parents, educators and health care professionals agree that the reason to debate how to care for developing feet is that foot and postural pain, suffering and deformity has increased to a rate that is alarming. Calls for re-examining how we house our kid’s feet to prepare them for a healthier, more productive life are coming from more diverse locations and they are getting louder.
Historically, children’s feet have been left alone to make their own way in the world, until they either develop pain, deformity or performance issues as juveniles or young adults, or they pass on to being adult feet too often destined for bunions, or knee and low back pain or performance issues.
Kids' shoes, until recently, were developed, marketed and promoted by the shoe manufacturing industry to parents, educators and health care professionals, preparing our kids to accept the tight, heeled, unhealthy but stylish shoes they are marketing for adults to wear.
In the last year or two, the pendulum has swung in the opposite direction, with
refreshing entrees into the pediatric footwear marketplace like VivoBarefoot Kids, Merrell Kid’s and Pediped Shoes that offer generous, zero heeled, flexible shoes claiming to prepare their users for a “barefoot”, healthier, stronger and more injury free foot and postural future.
The current marketplace for kids shoes is wide open but polarized into two biased self funded groups, served by biased blogs and social media, calling for society to choose between them without a middle ground.
It is my opinion that the key caveat that is overlooked in the Children’s Shoe debate is that like it or not, all feet, even one's left and right feet are different, mechanically. The foot type that we inherit has huge influence over our functional lives from birth until death, but the pundits view all feet as if they behave alike mechanically when it comes to developing shoes. Summarily, the starting platform for examining kids feet is unrealistic, because what is good for one foot type of feet is often bad for others and it is fostering predictable future foot and postural pathology that could be avoided.
I opine that we need to interject some biomechanical sense into the mix in order to temper and centralize the debate to consider the variations that exist among us all for the benefit of our kids.
Let’s start with some information, thoughts and theories that deserve consideration when visiting shoe gear for developing feet (defined as: the human foot until bone growth ceases), biomechanically.
Horses race for the Triple Crown at 3 years of age.
Humans can barely complete a short slow jog.
Antelope run away from an attacking cat days after just being born.
Humans stay relatively still and weak for almost a year before taking an erect step.
Summarily, parents are not educated or prepared as to how to house their children’s feet for future health and fitness.
We are a society that must protect and prepare our young until they can become productive and when it comes to their feet, the shoe industry has not put enough emphasis on function and fitness and instead place children into adult shoes manufactured in children’s sizes and start introducing tight fitted and stylish shoes too early and aggressively.
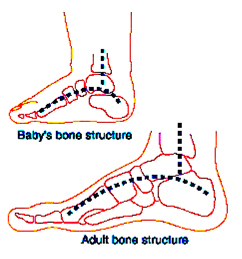
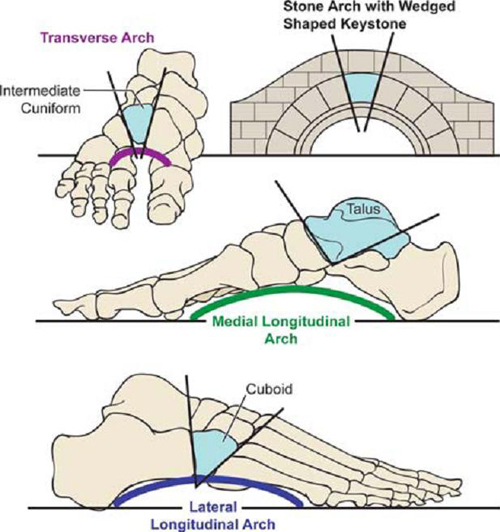
Until one year of age, infants have a bony pedal arch structure not unlike an Architectural Arch. Two equal pillars and a central keystone.
In fact, from the age of seven on, the distal bones (the forefoot) grow faster and longer than our proximal bones (the rearfoot) allowing our muscles to develop lever arms that once trained, form a flexible tie beam that can support our bony truss and allow it to perform tasks such as lifting, moving, walking and running well posed. Problems occur at this time if the tie beam doesn’t strengthen as fast as it needs to in order to maintain pedal biomechanical health.
 |
| |
In addition, biomechanically, some feet are weak in the back, some in the front, some in both and some in neither. Furthermore, our weaknesses show up at different ages with varied consequences for each of us. The current gold standard for profiling feet is called the wet test. This examines wet feet for the footprint they leave on the ground grouping them into high, normal and flat arches. This method falls short because it doesn’t define where the arches are failing and it offers no direction for treatment. I believe what we need is a new profiling system targeting the locations of the foot that are collapsing for each of us so that we can be correctively supported and strengthened starting with shoes that are developed foot type and age specific.
The Old Testament states that a boy becomes a man at thirteen (the Bar Mitzvoh in Judaism), the army drafts soldiers at eighteen (when bone growth ceases). These ages define periods in our development where the differences that exist within us all help direct us to our “life calling” when it comes to work, play and lifestyle.
One, Seven, Thirteen and Eighteen are ages where decisions should be made that take a homogenious population and diversify it into a heterogeneous civilization.
In light of these facts, it seems reasonable to state that at least until seven, children’s feet, as a rule, should be in spacious, flexible, light, foot shaped shoes, or barefoot.
My focus has been to profile all human feet to place them into smaller groups using morphology so that they can be studied more purposefully. This has led me to the conclusion that depending on ones biomechanical makeup, children’s feet should live in shoes that magnify the strengths and overcome the weaknesses that exist in them. This goal can be best met by developing shoes, temporary props and training programs starting with a foot type-specific platform. This means changing kids shoes and the current orthotic model which advocates their permanent and almost universal use.
If we go back to the architectural parallel, some feet collapse in the back half, some in the front one, some in both and some in neither. When feet are profiled, they can be classified into types, creating a starting platform for each type that can be applied for developing shoes, footbeds, exercise and training programs and to use this as part of the decision making process when choosing lifestyles.
Juvenile Tie Beam Expansion
To better explain my point, there are some children that develop pathological flat feet and bunions at a very young age. Their feet are growing like those of other children but in addition, they are getting longer, wider and flatter due to mechanical collapse coming from weakness in the flexible tie beam. This pathological scenario is known as Juvenile Tie Beam Expansion (JTBE) and unless treated early, it leads to a lifetime of foot and postural pain, suffering and deformity. Props, training and exercise or in severe cases, reconstructive foot surgery is in order for these kids.
My position therefore, is that children, and depending on their inherited foot type, should be prompted to wear minimalistic shoes as much as possible with added custom, foot type-specific props and/or training if they have JTBE until age 13 and then at that age, taking into consideration parental, societal, physiological and individual factors, start to introduce tighter, more stylish toeboxes and higher heels realizing that at that moment, they are sacrificing their health and foot and postural functional future depending on lifestyle selection.
At age eighteen, or when bone growth ceases, feet should be supported and trained where necessary, foot type-specific to prevent Adult Tie Beam Expansion (ATBE), a lengthening, widening and flattening of the foot after bone growth ends, with a goal to develop an exercise, activity, shoe and prop wardrobe that will maintain performance, quality of life and lifestyle until death.
It is my goal to influence the decision making of all sides of the children’s shoe debate that a professional, state of the art biomechanics paradigm should be developed as a starting platform in order to develop a new generation of kids shoes designed for health, protection and prevention that will produce a generation of wearers that are stronger, more productive and more injury free throughout their adult lives.
This eZine was made possible through the support of our sponsors: |
|