
What Kind of Podiatrist Do Today’s Residents Want to Be? – Survey Results


We currently offer a single path in podiatric education designed to train advanced foot and ankle surgeons. All podiatrists currently do three years of residency training heavily weighted in surgery, designed to produce advanced foot and ankle surgeons. Our education system has evolved in the last 50 years to put a heavy weight on surgical training. Even our basic values and self-image have evolved such that we tend to consider the podiatrists who do the most advanced surgery to be better and more successful podiatrists.
Advanced Foot and Ankle Surgery vs General Practice Podiatry
One BIG factor that distinguishes medical and podiatry schools is that medical schools offer a multi-track education, where students can become medical doctors or surgeons, internists, psychiatrists, cardiologists where currently, podiatric residency education has now been standardized to train us all to be advanced foot and ankle surgeons. The issue is that many of us are not inclined to be advanced foot and ankle surgeons, but are instead inclined to be great general practice podiatrists. We ALL don’t need to be advanced foot and ankle surgeons, so why are we putting all of us through this training? Most of us should be general practice podiatrists, because that is what best serves the public health needs. General practice podiatrists handle most of what patients need. Only a small portion of podiatry patients require advanced foot and ankle surgery.
Have We Lost Our Balance?
For some time now, I have questioned why we put ALL podiatric residents through an advanced foot and ankle surgery residency program? I believe that the momentum of our energized, righteous push to become THE advanced foot and ankle surgeon has led us to an over emphasis on advanced foot and ankle surgery, and a relative neglect of what most podiatry work is, which is office-based general practice podiatry.
Restoring the Balance
I have proposed that we re-assess how the structure of podiatric residencies can be changed to better meet the needs of ALL residents, as well as the needs of the profession, and the public health. Toward this goal, I have proposed a dual track 3rd year for podiatric residencies, in which we divide residents into a track for advanced foot and ankle surgery and a track for general practice podiatry.
This is a particularly important time to discuss podiatric residency education, as many of you know that the CPME has convened its Ad Hoc Committee to review the CPME 320 document, the requirements for podiatric residency programs. The review, reconsideration and possible alterations to this document will shape the nature of podiatric residency education until the next revision, and will go directly to the heart of what we’ve been discussing: the QUESTION – “What Kind of Podiatrist Do Today’s Residents Want to Be?” and “Do the Current Three Year Residency Programs Prepare All Podiatrists Best for the kind of podiatrist that they want to be?”.
The Survey Results – What do Current Podiatric Residents Want?
I wondered how current podiatric residents feel about these issues, so I designed a Residents Survey to assess their views on this topic and invited about 1,000 current podiatric residents to take it. The results were very interesting and I want to share them with you in the interest of moving this discussion forward.
I purposely gave the residents ample opportunity in the survey to write narrative explanations as to what exactly they want and why they want it, so reading through their responses reveals quite a bit of depth and nuance. This helps us to understand how they feel and what they want.
The Results
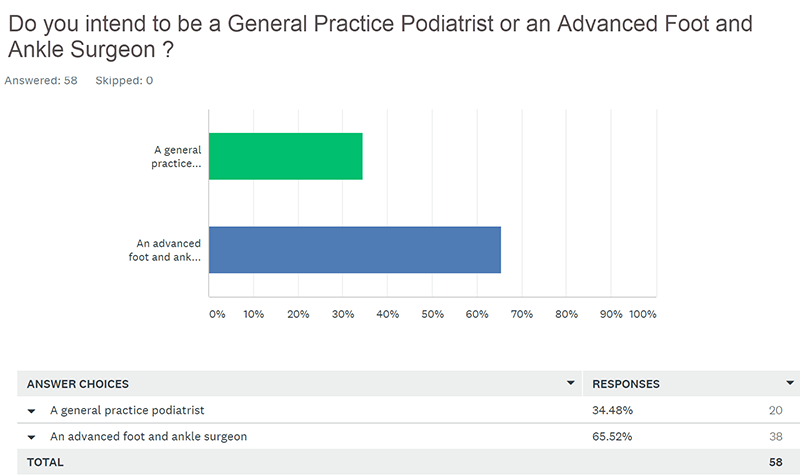
In reading through the responses, it’s clear that not all podiatric residents are alike and not all want to be advanced foot and ankle surgeons. When asked what type of podiatrist they intend to be, 66% of current podiatric residents stated that they intend to be advanced foot and ankle surgeons, with 34% stating that they intend to be general practice podiatrists.
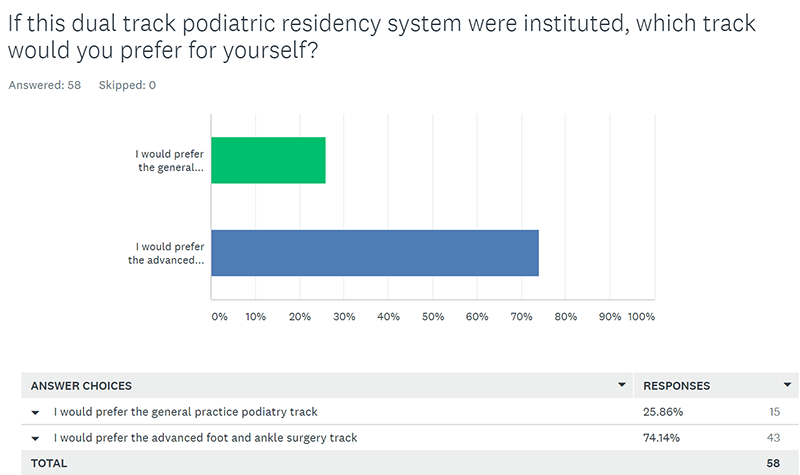
Then we asked them specifically about what track they would choose for their 3rd year of residency education if both an advanced foot and ankle surgery, and a general podiatry practice track were offered. The responses show that, 74% or about ¾ of them would choose the advanced foot and ankle surgeon track and 26% or about ¼ would choose a general practice podiatry track. So 8% of the 34% that intend to be general practice podiatrists still want the training in advanced foot and ankle surgery. But the results show that we could be putting as much as ¼ of residents through a 3rd year of advanced foot and ankle surgery training that they don’t need or want.
8% of the 34% of podiatric residents that intend to be general practice podiatrists still want the training in advanced foot and ankle surgery
What Do We Make of These Results?
It can be argued that more education is always better…that even the 26% of current residents who do not aspire to be advanced foot and ankle surgeons are better off going through this training anyway. I would argue against that – for two reasons. First, those going on to general practice would be better served by doing higher volumes of office/clinic based patient care during their 3rd residency year, of the type and variety that they’ll be doing in practice. Secondly, surgical cases are being done by these general practice podiatrists that should be adding to the case volume of those going on to be advanced foot and ankle surgeons.
What Surgical Procedures Do General Practice Podiatrists Need to be Competent in?
To be clear, I am not advocating for taking away a podiatrist’s scalpel and replacing it solely with a prescription pad. We will ultimately need to decide what surgical procedures general practice podiatrists need to be competent in. I am merely trying to maximize the usefulness of the 3rd year of residency training, and compelling the profession to recognize that it doesn’t serve our best interests as a profession, nor the best interests of public health, for ALL podiatrists to be trained as advanced foot and ankle surgeons. We should recognize that most of what needs to be treated in a podiatric practice does not require an advanced foot and ankle surgeon. Note Question 6, “Which procedures do YOU think should be included in the list of those that a reasonably well-trained General Practice Podiatrist should do?”. I had suggested, Surgery on the digits (including HAV, hammertoes, etc), STJ arthroeresis, nail surgery, I&D abscess, and excision of soft tissue mass. The residents’ responses were all over the board, with some of them suggesting that procedures as advanced as Brostrums and ORIF of ankle fracture should be included in the training of the general practice podiatrists. I think there is some fear and trepidation involved with this discussion, as no one wants to be denied training during residency in any procedure that they may want to do in practice. This is not about taking away training from those who want it. It’s about not wasting training on those who don’t want it and won’t use it.
Most of what needs to be treated in a podiatric practice does not require an advanced foot and ankle surgeon. It doesn’t serve our best interests as a profession, nor the best interests of public health, for ALL podiatrists to be trained as advanced foot and ankle surgeons.
For those of you involved in podiatric residency education, I feel I need to acknowledge that I have the greatest respect for the work that you do in running your programs, and know that implementing anything like what I propose will be difficult. Change is ALWAYS difficult. Just as a patient accepts post-op pain as a consequence of the good that the surgery does for them, I think we need to consider whether a change in our residency training would result in enough improvement in the years ahead to warrant the difficult job of implementing it.
Additional Reading
A New Direction in Podiatric Residency Training – Dual Track Third Year
Is Podiatry a Surgical Specialty or is Surgery a Sub-Specialty of Podiatry?
Practice Perfect 644 - Is Podiatry a Surgical Specialty? – A Response by Jarrod Shapiro, DPM
Further Discussion on Whether Podiatry is a Surgical Specialty, and Whether We Should go to a Dual-Track Third Year in Podiatric Residency Programs
Alan Sherman Submitted Comments to CPME 320 Ad Hoc Committee on the Structure of Podiatric Residency Education

Comments
There are 4 comments for this article
Alan, I applaud your efforts to draw attention to the fact that our current podiatric residency training has one focus: advanced foot and ankle surgery. What is eye-opening in your survey is that the majority of current residents (92%)actually believe that this will be their career option. The reality is that a very small percentage will spend 100% of their time performing foot and ankle surgery. Very few will end up being pure foot and ankle surgeons. The vast majority will end up working in a clinical setting where they will have to evaluate, diagnose and treat a broad spectrum of foot and ankle pathologies and the preferred initial treatment for these conditions will be non-operative interventions. The current curriculum for 3 year podiatric surgical residency training provides minimal opportunity to evaluate and treat all foot and ankle pathologies in a non-operative fashion. As Jarod Shapiro has recently pointed out, there is virtually zero training in biomechanics, physical medicine, rehabilitation and orthotic therapy. I submit that our fellowship trained orthopedic foot and ankle surgeons have better training in this regard because they spend considerable time working in hospital based outpatient clinics where they have responsibility for treating their own patients. In this regard, I question how a "office-based general practice" podiatric residency program could ever be implemented given the lack of outpatient clinic exposure currently available in today's podiatric residency programs? Furthermore, what practitioners would be adequately trained and credentialed to serve as attendings at such a program? The challenge is daunting, especially considering that the vast majority of students and residents have no interest in this novel, and very valid idea.
Thanks for your kind affirmations and further thoughts, Doug. My assumption is that the additional clinical training in general podiatric practice would take place in a combination of clinic settings, based on what is available or can be set up for each program. An expansion of hospital based clinics in some cases, and Directors/Attendings opening up their offices on a more organized, curriculum based basis, would provide the main training for the general practice 3rd year track. I never even whispered that this would be easy, because I know it won't be. But I'm gratified that almost every single one of the many dozens of podiatrists I have spoken to about all of this during the last 3 years has agreed that it is needed and would provide an improvement, both for podiatry students/residents, and for the public health. I think you overstated (92%) the number of residents responding to the survey that they expect to be advanced foot and ankle surgeons. It was 65% from the survey. Unless I am misunderstanding you. If you agree and can change it above, please do so. I look forward to seeing you next.
Alan, Thank you for noticing my error in assuming that 92% of the survey participants want to be advanced foot and ankle surgeons. Yes, the survey indicates that 65% of current residents aspire to be advanced foot and ankle surgeons. Of the remaining 34%, 8% still want advanced foot and ankle surgical training. I still question why 73% of current residents would want to devote the vast majority of their post graduate training focusing on a discipline which will NOT be the primary tool in their clinical arsenal. This is an astounding finding in my opinion. It should be noted that this survey had an extremely low response rate ( 58/1000) so one could question whether this small group actually represents the majority of current residents? Either way, I want to re-state my primary purpose in responding to this article. Currently, our podiatric residency programs do not provide enough time or training in the implementation of non-surgical treatment interventions for lower extremity pathologies. Providing those treatments will be the primary duty of the vast majority of residents when they enter employment as podiatric physicians.
Alan, Your commitment to the podiatric residency training has been well recognized and appreciated over the years. And I also laud your thoughtfulness in trying to bring more reality into the podiatric training process. In considering your comments, I believe we have to look at the history of our profession to find out why we are in the current state. It is important that we not go backward in trying to solve the current problems. 1. Podiatry developed outside the framework of the allopathic and osteopathic professions. We were not taken seriously as doctors and did not have access to hospitals until we became surgeons. CCPM, under the leadership of Dr. Pierce Nelson, took a giant step forward by establishing a hospital as part of their campus. This started putting economic pressure on the hospitals in their area as foot surgery was seen by administrators as a highly profitable source. Today, podiatrists have become part of a large percentage of hospital staffs throughout the country, providing not only better medical care than ever before, but also providing good financial income for hospitttals. 2. The ABFAS was the first certifying board, which was needed by hospitals to say that those who were doing foot surgery had adequate expertise. Being the oldest board, it became the only option for podiatrists to certify in order to gain hospital access. Today the ABFAS is the most powerful certifying board because of they have the largest number of diplomates. 3. Because not all DPMs could become certified by ABFAS for either lack of interest or opportunity, the ABPO and then the ABPPM were established to increase expertise and certification in those areas that were considered non-surgical. These two boards, thank heavens, decided that they could merge into one board, the ABPM. The ABPM continues to make advances and increasing its influence by increasing numbers. As they also require a certain amount of surgical expertise, it is becoming a more viable option to pursue certification by young practitioners and those who want to do some surgery that is of a less complicated nature. 4. With the development of three different boards, an alphabet soup of podiatric residencies were established. This alphabet soup ended up confusing outside sources as well as dividing the profession into a "haves" and "have-nots." Those students who graduated in the top of the class got the PSR-24 or PSR-36 programs and those at the bottom of the class got the PPMR programs. It created an arrogance by the haves as those who didn't have the PSR-24 or better struggled more to establish strong practices after training. The reasonable course was to create a stronger podiatric profession by having a single 3 year residency program. The establishment of this put many of the small residency programs out of business, many of which had very strong clinical non-surgical training and helped the young physician figure out that a majority of foot problems don't need surgery. 5. With the establishment of a single 3 year residency, there still was a two tier system set up, one leading to certification in rearfoot surgery one without. However, almost all programs have adopted the RRA tier because it is difficult to attract top quality students to a program that does not have RRA. 6. ABFAS continues to set minimum activity volumes that are not based on any type of evidence, only on average volumes. Who can say that it takes 80 digital surgeries to become competent in digital surgery, but only 60 first ray procedures to become competent? And only 50 rearfoot surgeries to become competent in all types of ankle trauma and reconstructive surgery? Since ABFAS is the major driving force in the residency model, shouldn’t ABFAS set surgical MAVs based on evidence of competence? Should ABFAS quit demanding a certain number of surgeries during residency training, and instead base certification on demonstrated competence, no matter what the tier of residency training is? Who cares if competence is developed during residency training, during fellowship training or even after several years of working with someone who is very competent? Competence is competence, no matter what the source of training. This would markedly decrease the pressure on residency programs to provide exotic surgeries or even surgeries which will never be utilized in an average practice, and instead focus on developing patient centered competence. 7. ABPM has become more popular in recent years because of their offering certification at an earlier stage of the young practitioner's career. ABPM has set MAVs for biomechanical examinations during the residency program, however any reviewer for CPME will tell you how difficult many programs find in meeting the MAV. This writer has a lecture on this particular forum in how the biomechanical examination helps a surgeon decide on the best flatfoot surgery to perform. If every flatfoot surgery required a biomechanical examination as part of the pre-op workup, the biomechanical exam MAV would be much easier to meet. Likewise if a biomechanical exam MAV was required before any bunion surgery, this requirement would be much easier to meet. Considering these aspects, instead of taking a step backward in time by making more division in the profession by having a two tier residency program, it is time to consider the following proposals: 1. ABFAS and ABPM need to consider uniting as a single board. As a single board, various certifications could be offered, including certifications in general medicine, physical medicine, and various surgical options. Practitioners would be able to continually add certifications to their resume throughout their career. The board certifications would be based on demonstrated competence, not on the type of residency one completed. 2. MAVs for residency programs should be established on evidence. The profession clamors for evidence based medicine, but who is clamoring for evidence based education? 3. Residency programs should become more focused on following patients from pre-op, through workup, through surgery and post-op care. Instead of having MAVs for each little category, MAVs should be set for following patients with various pathologies over a period of time. The current system is now set on training surgical technicians, not on treating patients in a wise and thoughtful manner. In summary, podiatric medicine has made great strides in the 40 years that I have been part of it. We have solved many problems. Most podiatrists, especially new practitioners, now have access to hospital practice and also board certifications. This is because of the selfless sacrifices of so many of those who have gone before in making the profession better than they found it. Today the trainers of students and residents continue to make the sacrifices of putting the interest of young practitioner’s futures ahead of their own interests. I applaud the efforts of all who do so. Let us continue to work together to make the profession more united and more competent.