

Practice Perfect 724
Offweighting the Heel with a Simple, Low Cost Modified Posterior Splint
Offweighting the Heel with a Simple, Low Cost Modified Posterior Splint


In the hospital, one of the challenges as a podiatrist is properly offweighting the heel. For example, in patients with decubitus heel ulcers, it can be very challenging to remove the pressure that caused an ulcer in a bedbound patient. Various products are available, from foam and inflatable protectors – which usually do not work particularly well – to the well-known ankle foot orthosis or multipodos boot, which is much too expensive for all but the most generous hospitals to keep on the shelf. As a result, I too often see patients in the hospital with heels elevated on pillows, another poor offweighting method. Additionally, in the outpatient environment, private insurances may not cover expensive but high-quality devices.

Good Solutions at High Cost
This has been such an issue that Roukis, et al pioneered the use of the “kickstand” external fixator to offweight reconstructed heels with soft tissue defects,1 using a delta frame to essentially suspend the foot off the bed. Similarly, Castro-Aragon also used a kickstand modification to a delta-type external fixator to prevent heel ulcers.2 These expensive offweighting modalities are very creative, but the cost is prohibitive for average situations.



A New Technique – Effective at Low Cost
Out of necessity, I invented a simple, low cost modification to the posterior splint to offweight the heel. First, apply a posterior splint in whatever standard way you choose with any dressing (Figures 1 and 2).



Then place an ACE wrap or roll bandage of your choice between the area of the heel to be offweighted and the posterior splint itself (Figure 3).


Secure the splint with bias or ACE wrap. Allow the splint to harden completely while maintaining proper foot to leg position. Then remove the roll bandage. Note the space created, allowing the heel to hang without pressure (Figures 4 and 5).

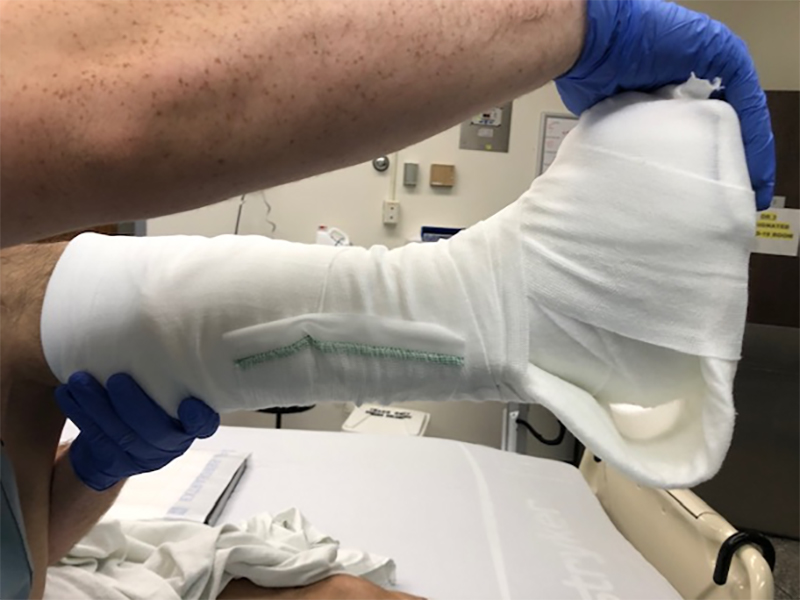
Confirm that the splint hardens completely before letting go to prevent flattening. Additionally, be cautious not to create too sharp of a transition between the flat portion of the splint and the curve of the offweighting area to prevent excessive focal pressure. I’ve found this method to be highly effective to float the heel (or any other area that might come in contact with the splint, but it should not be used to allow weightbearing. Finally, using a longer splint and folding it back on itself will create a stronger splint when needed.
I hope all who read this find this method to be a useful tool to help with your patients.


-
Roukis TS, Landsman AS, Weinberg SA, Leone E. Use of a hybrid “kickstand” external fixator for pressure relief after soft-tissue reconstruction of heel defects. J Foot Ankle Surg. 2003 Jul-Aug;42(4):240-243.
Follow this link -
Castro-Aragon OE, Rapley JH, Trevino SG. The use of a kickstand modification for the prevention of heel decubitus ulcers in trauma patients with lower extremity external fixation. J Orthop Trauma. 2009 Feb;23(2):145-147.
Follow this link
Major Sponsor



















Comments
There are 0 comments for this article