

Practice Perfect 788
How Much Medicine Does a Podiatrist Need?
How Much Medicine Does a Podiatrist Need?


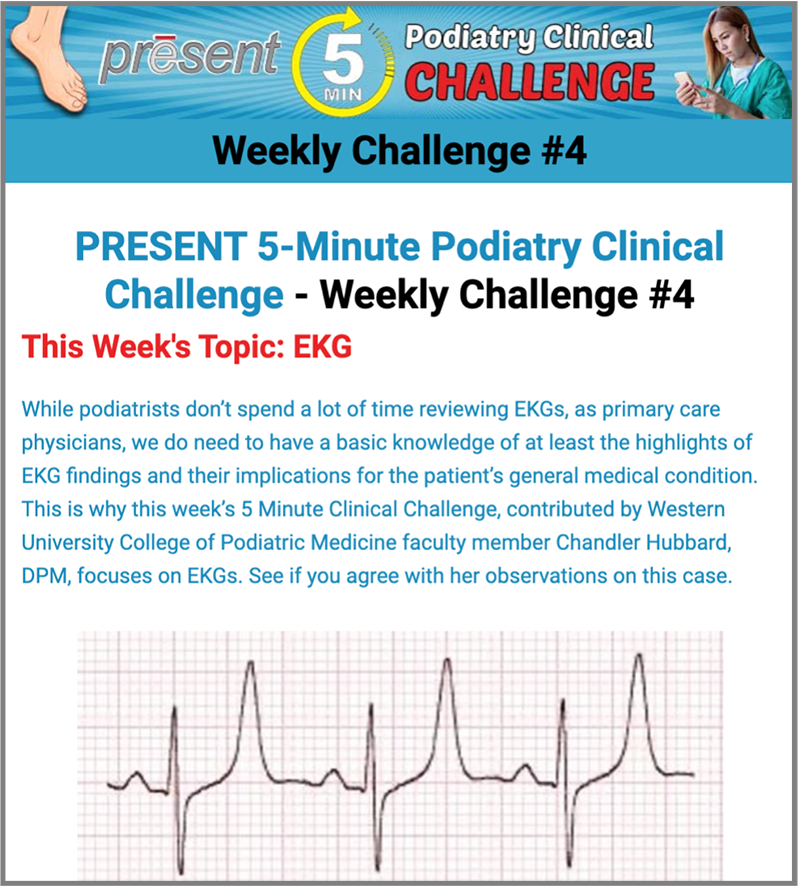
This past week’s PRESENT 5-Minute Podiatry Clinical Challenge about electrocardiology-related medicine, created by Chandler Hubbard, DPM, brought some interesting responses from participants. First of all, if you haven’t logged on and tried the challenge I strongly suggest doing so. It’s a fun quick way to test your knowledge. The correct answer explanations are well-cited and provide great opportunities to learn.
The question this edition seemed to spark was this: “Is reading EKGs something podiatrists really need to know?” If we broaden this question to “how much medicine should a podiatrist know?” my simple answer is, as much as possible.
How much medicine should a podiatrist know? As much as possible and as much as other surgical subspecialists.
Really, Shapiro? Podiatrists need to know as much medicine as possible. Yes, we do! Let’s discuss a few reasons why this is important and consider real life examples to illustrate these points.
Are We Physicians?
First, I’ll posit the argument that it’s simply good medicine and better podiatry. For many years, podiatrists were “experts of the foot and ankle.” Recently, things have changed. For many of us, we would rather be described as physicians who specialize in the lower extremity. We’re more than foot doctors. This more holistic view requires a comprehensive education and improved understanding about the rest of the patient, which is now occurring at our podiatric medical schools.
Podiatrists have long been “experts of the foot and ankle.” But we’re more than “Foot Doctors”. We are physicians….
A common podiatric example of this is plantar heel pain. A physician who is ignorant of the potential contribution of the lumbosacral spinal complex to foot pain may misdiagnose a patient’s heel pain. Similarly, ignorance of vascular physiology may lead one to miss claudication or ischemic rest pain in a patient with lower extremity pain. These are common extra pedal causes of perceived foot pain.




Examples From Just This Week
The next issue is, like it or not, you’re likely to be questioned about medical issues for your patients by other doctors on the team. This is especially true if you work on patients in the hospital. During the week I’m writing this editorial, I’ve been on call seeing quite ill patients in two different hospitals. For each of these patients, I’ve received questions from nurses and other physicians about topics such as anticoagulation (should we stop the heparin drip on this patient?), blood sugar control (this preop patient’s preop blood sugar is 340 mg/dL; what do you want to do?), and – pertinent to last week’s clinical challenge – labs, blood gases, and EKG findings in a patient with bradycardia during the perioperative period. Without having a reasonable understanding of these topics, I would never have been able to interact properly with the rest of the medical team.
Now, I’m not advocating we practice outside our particular states’ scope of practice or that podiatrists should be overall general medical experts, but the expectations from the rest of the medical community is that anyone calling themselves “doctor” should have a reasonable medical background in a manner similar to other specialists.
It is simply better patient care to have a more comprehensive understanding of medicine. As an advocate for our patients, it behooves us to watch out for potential medical problems and not simply rely on other physicians. And this, my friends, is where Dr Hubbard’s questions regarding the EKG and findings consistent with hyperkalemia are spot on appropriate for us to know. Since the most common complication during surgery is related to cardiac disease, we must have a strong understanding of the EKG and review it before surgery as part of a comprehensive risk assessment before surgery.
Since the most common complication during surgery is related to cardiac disease, we must have a strong understanding of the EKG and review it before surgery as part of a comprehensive risk assessment.
I can’t recall a time when my understanding of medicine was not helpful. Is it somehow better not to understand that lower extremity edema may result from cardiac, renal, or hepatic disease in addition to venous pathology? Would we be better podiatrists if we didn’t understand the significance of a glycosylated hemoglobin of 9%? Are we somehow doing our patients a favor by not knowing what ST segment elevation is or, as we learned from the most recent 5-Minute Clinical Challenge that tall, peaked T waves is a common finding in hyperkalemia and highly dangerous?




When has ignorance ever been a good thing? Never. Keep participating in the PRESENT 5-Minute Podiatry Clinical Challenge and gain the power of knowledge.


Major Sponsor




















Comments
There are 0 comments for this article