

Practice Perfect 903
Are IPKs Just Warts?1
Are IPKs Just Warts?1


When I first started podiatry school, I was taught that intractable plantar keratomas (IPKs) were “blocked sweat glands.” This etiology of these painful hyperkeratotic lesions has been long debunked, but there continue to be questions about the etiology – and thus treatment of – this small but painful problem. A new study lends evidence that these keratomas are actually related to verruca.
Before we get started, I’ll make one clarifying point: we’re not speaking about the somewhat more diffuse tyloma but rather the hyperkeratotic lesion with a central core, the classic IPK.




Hot Off the Presses!
Alou, et al. performed a prospective observational trial “to determine the presence of human papillomavirus (HPV) in patients with intractable plantar keratosis (IPK) by comparing the histopathological findings of biopsies.”1
In a consecutively sampled group of patients, three specimens were taken from a plantar foot IPK lesion in otherwise healthy patients with an at least 3-month history of these lesions. The specimens consisted of a skin scraping and two 2-mm punch biopsies. One of the punch samples was sent for histopathological analysis and the other two samples for PCR testing.
A total of 51 patients (mean age 52 years and 62.7% female) participated. All of the lesions were located directly plantar to a metatarsal head, and the 3rd metatarsal head was the most commonly affected, although all metatarsal heads were involved.
Here’s what they found:
| Study Type | Verruca (HPV detected) | Keratosis |
| Histopathology | 35 of 51 (68.6%) | 16/51 (31.3%) |
| PCR biopsy | 49 of 51 (96.1%) | 2/51 (3.9%) |
| PCR skin scraping | 42 of 51 (82.4%) | 9/51 (17.6%)* |
*In 7 of the skin scraping samples PCR failed to confirm verruca where the deeper punch biopsy confirmed it.
Before we discuss the overall significance of these findings, it’s important to review the quality of the tests they performed. As you can see from Table 2, taken directly from Alou and colleagues’ paper, PCR testing had a moderately high 71% positive predictive value (correctly diagnosing HPV when it was present) and a 100% negative predictive value (correctly ruling out HPV when it was absent). On the other hand, skin scraping had much lower positive and negative predictive values. This tells us we should not use skin scrapings to diagnose the presence of HPV in an IPK. Deeper biopsy is the way to go, and it seems reasonable to suggest we should test using PCR as the gold standard- or a combination of histopathology and PCR if you prefer additional testing.
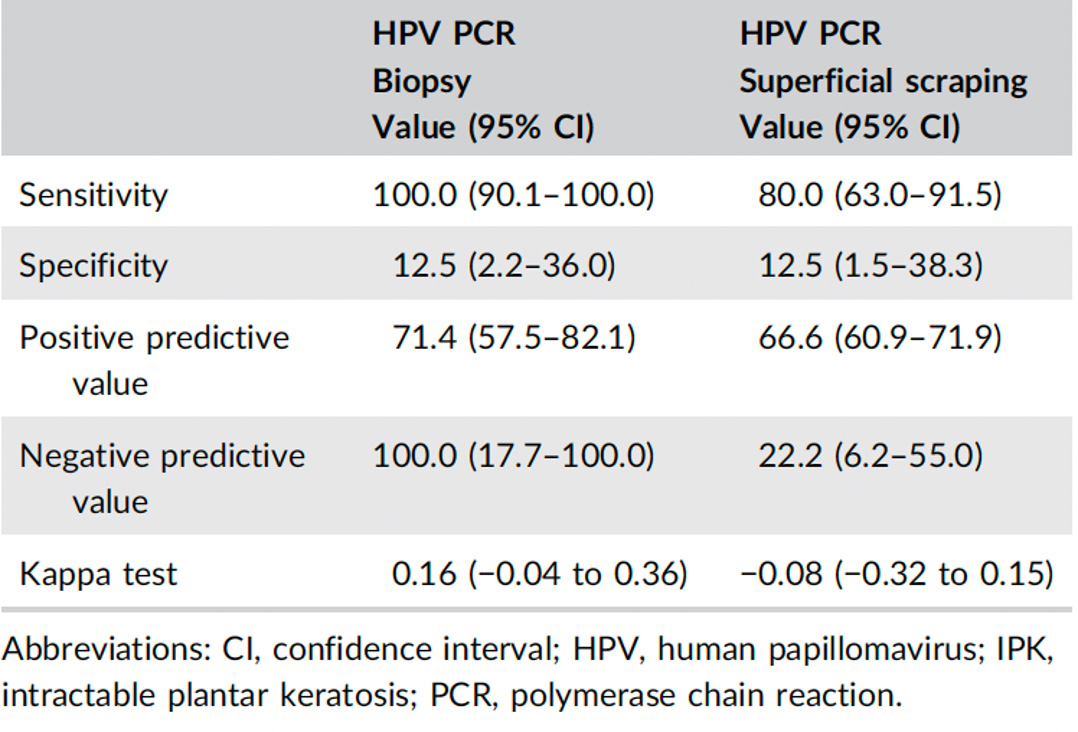
Table 2. Testing accuracy comparing PCR and surface scraping for possible HPV presence in plantar keratomasi.1
Now, based on the results, there is a strong argument that plantar keratomas are associated with HPV. Are these lesions warts or are they hyperkeratotic lesions that have become contaminated with HPV particles? This study can’t answer that question. This unknown is well recognized in a scoping review of a related topic (the current knowledge about surgical excision of plantar keratomas) by Reilly, Longhurst, and Vlahovic.2 They also recognize that more research is required to answer the question.
Clinically speaking, a number of these lesions are obviously not underlying a bony structure (this occurs perhaps 50% of the time in my experience, while tylomas are 100% of the time plantar to bony prominences). However, given the very high prevalence of HPV from Alou’s study, it would appear the most prudent course of action is to treat all IPKs as plantar warts, and lesion destruction or excision would be best.
However, we don’t know enough yet to rule out mechanical pressure, and it appears logical that pressure does have a significant role to play. If it didn’t, then why do we only see these on the plantar surfaces of the feet, many times directly under bony prominences? As such, my final take away is to treat these lesions with a combination of removal in some way (lesion destruction/excision) while offloading those lesions that are obviously underlying bony structures (padding/orthoses/surgical modification).




More research needs to be done to put this painful subject to bed, but for now, we’ll have to limp along with the knowledge that IPKs and HPV are in some way intimately related.
Best wishes.

Jarrod Shapiro, DPM
PRESENT Practice Perfect Editor
[email protected]

-
Alou L, Becerro‐de‐Bengoa‐Vallejo R, Losa‐Iglesias ME, Moreno J, Sánchez‐Gómez R, González N, Sevillano D. Strengthening the relationship between intractable plantar keratosis and human papillomavirus. J Med Virol. 2024 Feb;96(2):e29431.
Follow this link -
Reilly IN, Longhurst B, Vlahovic TC. Surgical excision of intractable plantar keratoses (Corns) of the Foot: A Scoping Review. J Am Podiatr Med Assoc. 2023 Nov-Dec;113(6):22-044.
Follow this link




















Comments
There are 1 comments for this article
I agree ! I have biopsy these IPK's for years with deep curettage excisional biopsy of lesions with local and nearly 100% are verrucae, not IPK. Do these minor procedures correctly, the risk of scar tissue is minimized and the lesion does not return. Some have a mechanical component, many don't...but they all are painful. More often than not, they have deep verrucae base that is hiding! It is surprising how many other Podiatrists have miss these golden opportunities to help these patients. Take the thorn out of the lion's paw , the word spreads, and more patients will come your way for with similar issues. I have 3 other Podiatrist's in our group that are in denial of this reality. They see these issues as only calluses, never biopsy, and the plane them down with their surgical 10 blade. They treat them as a nuisance calluses and they bill these patients for a visit every 10 weeks. It's the regular revenue they live on and not wanting to solve this elementary problem. We I see them, I solve their problems immediately and then they wonder why my practice partners treated them without definitive therapies, and I won them over for future patient referrals. I prefer my pathway for these issues. Most lawyers perpetuate an argument in lieu of solving a problem expeditiously. It about how many times we can bill a customer! Stiff necked people are in all professions. We need to open our eyes and humble ourselves. These benign lesions do not usually return when use apply a 10 second phenol application to the dermal wound base to kill the HPV micro remnants and then ETOH lavage of the wound base. I like the pearl of the PCR testing. Great article.